
Unusual anatomy of a mandibular second molar
Nonsurgical root canal therapy was performed on #31. During the procedure a mid-mesial canal was detected just lingual to the mesio-buccal orifice, via troughing with an ultrasonic tip and the aid of a dental operating microscope. Radiographs were taken to reveal an abrupt, midroot canal curvature and portal of exit in the furcal area. (See images 1-4)
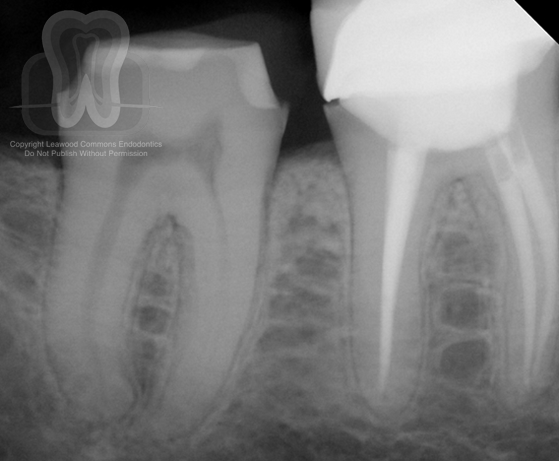
- Pre-operative radiograph
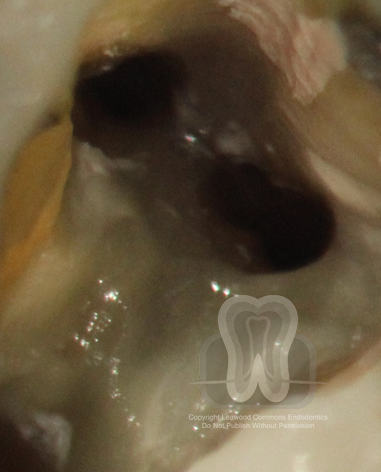
2. Intra-operative photograph demonstrating mid-mesial orifice

3. Intra-operative radiograph demonstrating mid-mesial canal and furcal terminus

4. Post-operative radiograph
- As in any case, detection and subsequent cleaning and shaping of all canals is vital for RCT success. As it pertains to mandibular molars, a clinician must always evaluate for the presence of a mid-mesial canal. Literature varies greatly regarding the prevalence of this anatomic feature (see attached articles for more information), but the current best evidence says it’s there roughly 20-40% of the time.
- So why does this matter? If left untreated, any tissue or necrotic debris left in the space may be sufficient to cause treatment failure. I particularly like this case because it illustrates another great point. Here, the mid-mesial canal doesn’t join one of the two other canals (as they do in the majority of cases); rather, it has a portal of exit in the furcal area. If that canal wasn’t treated, and it led to the formation of a lesion in the future, that would manifest as a furcal radiolucency on a root canal-treated molar…and we all know what that sounds like. Fracture! Dentists may assume this and prematurely extract a perfectly salvageable tooth.
- The take home message here is twofold: as a clinician, if you are performing RCT on a lower molar, be on the lookout for mid-mesial canals. This often requires the illumination an magnification of a microscope. As a diagnostician, don’t immediately assume that a furcal lesion on a root canal-treated molar is a crack.
- http://www.jendodon.com/article/S0099-2399(14)00786-9/
http://www.jendodon.com/article/S0099-2399(14)00900-5/pdf
We hope that you find these cases interesting. We’re sharing this case because we enjoy discussing all endodontic topics. If you are a member of the professional dental community with thoughts on this case, we would love to hear from you and add your contributions to this post.
Want to use our photos in a presentation or publication? Please email us and we’ll send you high-resolution original photos.